Fact Sheets
WABA ( World Alliance for Breastfeeding Action)
Wellstart International
SUPPORT FOR BREASTFEEDING IS CRUCIAL FOR INFANT HEALTH
IN THE AFTERMATH OF NATURAL DISASTERS
Under normal conditions in developed countries like the US, infants who are not breastfed are much more susceptible to infections and other illnesses. As a result, they are 3 times as likely to require hospitalization and 21% more likely to die in the first year of life. The costs of these excess illnesses are considerable for families, insurers, and taxpayers.
In the aftermath of emergencies like hurricanes Irma and Harvey, helping Mothers successfully initiate and continue breastfeeding is even more crucial. Children in vulnerable situations have special needs for the infection-fighting factors, the optimal nutrition, the reliable food source, and the comfort provided by breastfeeding. In contrast to powdered formula, which needs to be mixed with water, human milk provides ample hydration and spares infants exposure to water contaminated during the destruction caused by natural disasters. Direct breastfeeding also prevents the illnesses attributable to bottles and nipples “washed” in unclean water.
Most Mothers in the US want to breastfeed, but many quit sooner than recommended, citing lack of sufficient societal support as one key reason. Women warrant extra support during crises like hurricanes and floods. Every effort should be made to rapidly reunite and keep infants with their Mothers, provide space where they can feel comfortable nursing, and welcome moms to breastfeed whenever and wherever their babies show signs or hunger or distress.
Relief workers and health care providers should encourage mothers delivering during the crisis to breastfeed, help Moms initiate breastfeeding immediately after birth, recommend exclusive breastfeeding for approximately 6-months, and assist Mothers who recently stopped to restart breastfeeding (“relactate”).
Myths such as “stress makes the milk dry up” and “malnourished Mothers cannot breastfeed” must be dispelled with accurate information. Feeding the Mother is the safest, most effective way to ensure adequate infant nutrition during emergencies.
For more information about safe infant feeding in natural disasters follow the links at www.bfmed.org. The Academy of Breastfeeding Medicine (ABM) is a worldwide organization of physicians dedicated to the promotion, protection and support of breastfeeding and human lactation through education, research and advocacy.
——————————————————————————–
Breastfeeding in Emergency Situations
Breastfeeding is particularly important in emergency situations because of the increased risk of diarrheal diseases and other infections, inadequacy and contamination of complementary foods, and the bonding, warmth and care provided by breastfeeding which is crucial to both Mothers and children in emergency situations. The risks associated with bottle and formula feeding are dramatically increased due to poor hygiene, crowding and limited water and fuel. The role of breastfeeding is even more important in emergency situations where it may be the only sustainable element of food security for infants and young children. Exclusive and prolonged breastfeeding is often the only form of family planning available to women in emergency situations. Last but not least, women need validation of their own competence, BF is one of their important traditional roles that can be sustained during a stressful situation.
Misconceptions about Breastfeeding in Emergencies
Women under stress cannot breastfeed
Malnourished women don’t produce enough milk
Weaning cannot be reversed
General promotion of BF is enough
Human milk substitutes (infant formula and/or milk) are a necessary response to an emergency
Women under stress CAN Successfully Breastfeed
Milk release (letdown) is affected by stress. Milk production is NOT. Different hormones control these two processes. The treatment for poor milk release is increased suckling which increases the release of oxytocin, the letdown hormone. Research suggests that lactating women have a lower response to stress, so helping women to initiate or continue to BF may help them relieve stress.
Malnourished Women DO Produce Enough Milk
It is extremely important to distinguish between true cases of insufficient milk production (very rare) and perceptions. Milk production is relatively unaffected in quantity and quality except in extremely malnourished women (only 1% of women). When women are malnourished it is the Mother who suffers, not the infant. The solution to helping malnourished women and infants is to feed the mother not the infant. The mother will be less harmed by pathogens and she obviously needs more food. By feeding her, you are helping both the mother and child and harming neither. Remember that giving supplements to infants can decrease milk production by decreasing suckling. The treatment for true milk insufficiency is increased suckling frequency and duration.
A Mother who has weaned CAN Redevelop her Milk Supply
With enough nipple stimulation and milk removal, it is possible for women to re-lactate, that is to redevelop a milk supply. The stimulation can be provided by a willing baby or even older child, by hand expression and stimulation and/or pumping. The process may take several days or even a couple of weeks. Mothers need much encouragement, a reasonable supply of food and water and protection from stress to the extent possible. Babies, of course, need to be fed in the least hazardest manner until the milk supply returns.
Breastfeeding Women need SPECIFIC ASSISTANCE; General Promotion of Breastfeeding is Not Enough
Lessons learned in development programs show that most health practitioners have little knowledge of breastfeeding and lactation management; these lessons apply equally to emergency programs. Women who suffer through violent situations leading to displacement and emergency situations are at increased risk of breastfeeding problems. Mothers need help, not just motivational messages. Relief agencies and field workers need training on how to counsel Mothers to help them optimally breastfeed; how to assess proper positioning and suckling and remedy when needed and breastfeeding physiology. In some situations, breastfeeding specialists may be useful. Maternal perception of risk of breastmilk insufficiency is an important factor in a women’s decision for early termination of breastfeeding. These perceptions may be intensified by the stress of emergency situations. Our first concerns should be ensuring optimal breastfeeding behaviors, which may require the selective feeding of lactating women and trauma counseling for women who may believe they “don’t have enough milk”. Policies and services which undermine optimal feeding such as giving food supplements to infants <6 months and using bottles for ORS delivery, should be avoided. Successful breastfeeding will contribute to the restoration or enhancement of woman’s self-esteem, critical to her ability to care for herself and her family.
Human milk substitutes (infant formula and/or milk) are NOT always needed
Providing infants and young children caught in an emergency situation with substitutes for human milk is extremely risky. It should be undertaken only after careful consideration and full awareness of the problems that may result. Good guidelines exist on the use of human milk substitutes and other milk products in emergencies: the 47th World Health Assembly Resolution WHA 47.5 (May 9, 1994); UNHCR guidelines on use of milk substitutes (July 25, 1989); the International Code of Marketing of Breast-milk Substitutes, WHO (1981). Common elements of these guidelines are that human milk substitutes must be:
limited to special circumstances as defined in WHA 47.5;
guaranteed for the lifetime of emergency;
not used as a sales inducement (therapeutic feeding, never in general distribution);
accompanied by additional health care, water, fuel, and diarrhea treatment;
include plans for the re-establishment of optimal feeding from the outset of the emergency.

These guidelines should be disseminated and followed by all agencies working in emergency situations.
Optimal Feeding Practices in Emergencies:
Initiation of breastfeeding within one-hour of birth
Effective infant positioning (latch-on)
Frequent, on-demand feeding until 6-months of age
Exclusive, breastfeeding until 6-months of age
Continuation of breastfeeding after beginning the addition of appropriate weaning foods at 6-months of age
Sustained breastfeeding well into the second year of life or beyond
Increased breastfeeding frequency and continued feeding during illness.
Increased breastfeeding frequency after illness for catch up growth.
Originally prepared by Wellstart International’s Expanded Promotion of Breastfeeding Program (1996); revised and updated, 2004. For further assistance, consultation and/or training please contact Wellstart International at info@wellstart.org
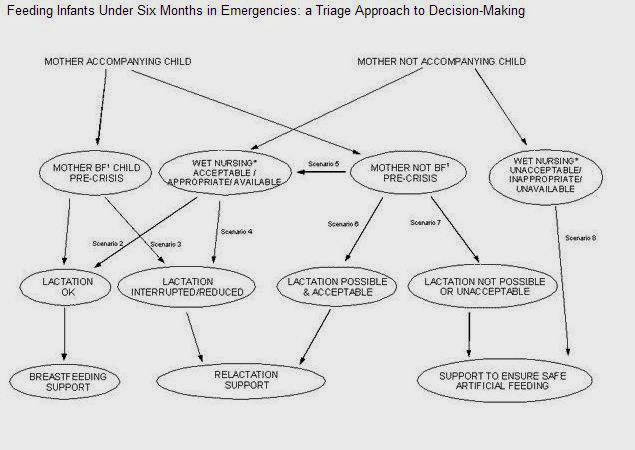
Emergency situations are usually initially confusing and chaotic. Determining who needs what is an essential early step. For protecting and supporting breastfeeding the first step is to identify infants who are or should be breastfed and further noting any infants who are temporarily or permanently without their Mother. Ultimately three groups can be established: one needing only breastfeeding support, a second requiring more intensive re-lactation help and a third in which substitute feeding is deemed necessary and will need to be very carefully managed and monitored.
See also: Homeopathic First Aid for Hurricane http://classichomeopath.com/homeopathic-first-aid-hurricane/
The triage diagram below may be helpful. It is from: Infant Feeding in Emergencies: Policy, Strategy & Practice. Report of the Ad Hoc Group on Feeding in Emergencies: May 1999 and has been made available by the Emergency Nutrition Network on their website: http://www.ennoline.net/ife/index.html
Breastfeeding in Emergency Triage Decision Making: